We find this difficult to talk about especially during these trying times. However, we feel it is important for all practices to know that HIPAA violations and fines have not disappeared during this pandemic.
Investigations take a long time and many practices think since they have not heard of small practices being fined that they are immune. Unfortunately, that is not true. Fines are smaller, but even the “small” fines hurt small practices. Could you afford $25K or $50K in fines?
The latest fine of $25K for ongoing HIPAA violations could have been more but the statute of limitations is 6 years. It was reported that they had failed to implement security rule policies and procedures, failed to provide their employees with security awareness and training, and they failed to conduct a thorough assessment of potential risks and vulnerabilities to the confidentiality, integrity and availability of the ePHI they held.
To read the full resolution agreement click here:
https://www.hhs.gov/sites/default/files/metro-signed-agreement.pdf
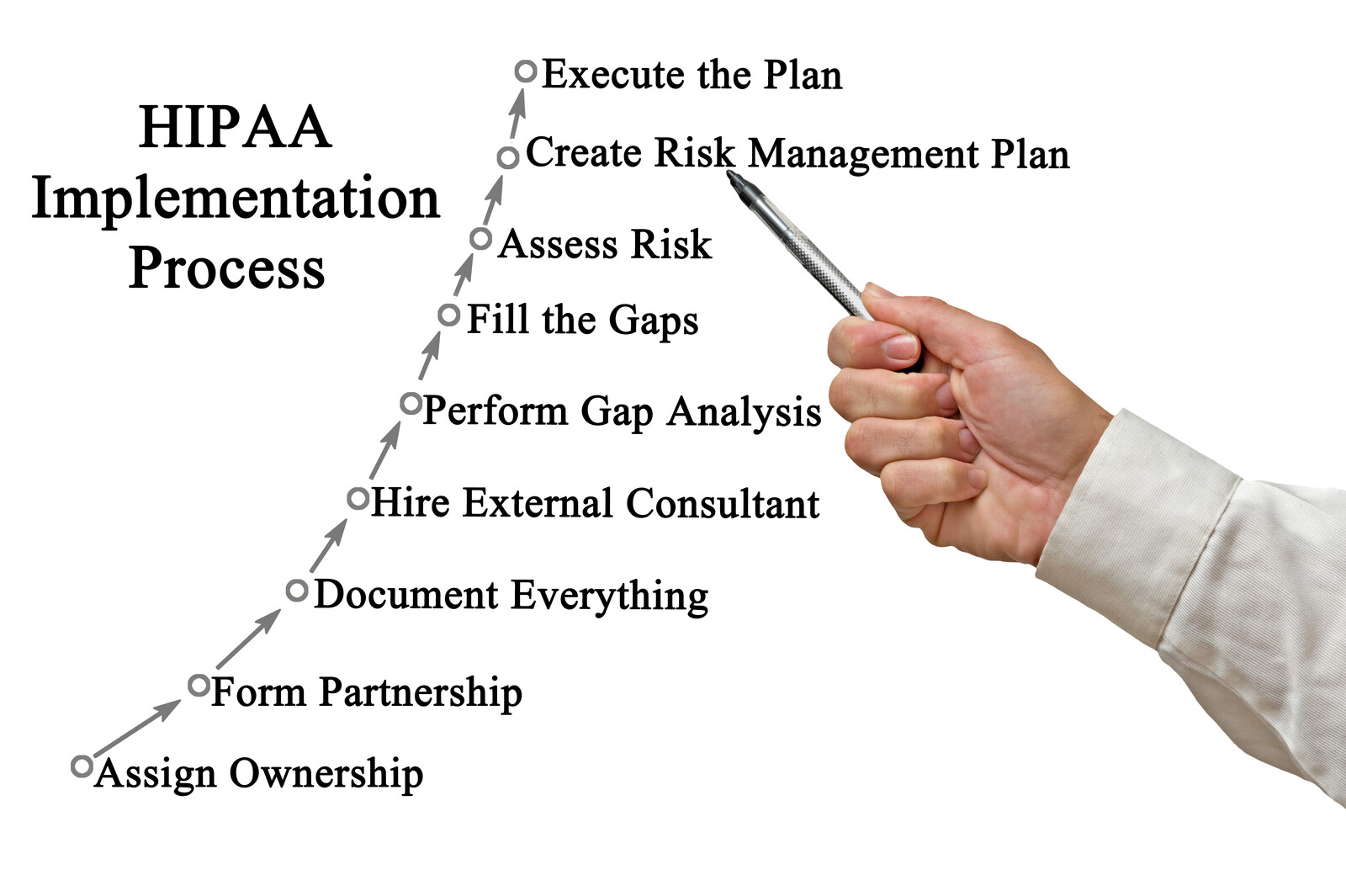
We understand that after you conduct the HIPAA risk analysis, the hard work begins. Implementing your HIPAA policies and procedures and documenting your risk management plan are difficult and there never seems to be enough hours in the day to complete this task. This is a MUST!
To find out more about how our automated HIPAA compliance platform can help your organization click here:
https://arismedicalsolutions.com/aris-hipaa-service-automated-platform/
Or to schedule a demo click the contact us tab and scroll down.
“Simplifying HIPAA through Automation, Education, and Support”







